





Attapadi, India’s first designated tribal block, nestled among the hills near Silent Valley National Park in Palakkad district, Kerala, is home to the Muduga, Kurumba, and Irula indigenous communities. The oft-discussed Kerala model of good health at a low cost received a jolt in 2013 when reports began to pour in about high levels of infant deaths among the indigenous people of Attapadi. 1 While Adivasi or Scheduled Tribes are the commonly used terms in India to denote those belonging to the indigenous communities, we have chosen to use the term 'indigenous' over the term Adivasi. The indigenous category focuses attention on the larger social and political determinants of well-being such as the continuing colonisation and expropriation of tribal lands, forests, and other resources by dominant groups. In using this term, we have followed the writings of Indian indigenous academic Virginus Xaxa (2012). 'Tribes and Development: Retrospect and Prospect'. In Social Exclusion and Adverse Inclusion: Development and Deprivation of Adivasis in India. Edited by Nathan, D. and V. Xaxa: 23–35. New Delhi: Oxford University Press. The response of both the centre and the state was swift. The-then union minister for rural development, Jairam Ramesh, visited Attapadi in 2013 as an emissary of the prime minister to take stock of the situation and implement relief measures.
Since then, every time there has been a spike in infant deaths, Attapadi has witnessed high-profile visits by politicians and key officials from the centre, who visit tribal hamlets, hold meetings with local officials, and announce corrective measures.
Several steps have been implemented to improve the well-being of the indigenous communities in Attapadi and prevent infant deaths among them. These have primarily depended on doing the following.
- Revamping the local health system by improving facilities, appointing more staff, and making all treatment free. A special scheme has also been introduced for pregnant women from the Muduga, Kurumba, and Irula communities in Attapadi.
- Addressing malnourishment through setting up community kitchens, nutrition rehabilitation centres, and a Millet Village scheme
- Restituting indigenous lands that have been alienated by setting up mechanisms to expedite the process.
Special financial packages have been launched to ensure that funding will not be a barrier to improving the health and well-being of the indigenous communities. Acknowledging that a key bottleneck in effective governance had been the lack of inter-sectoral coordination, a special mechanism under the sub-collector of Ottapalam has also been set up.
Health system in Attapadi
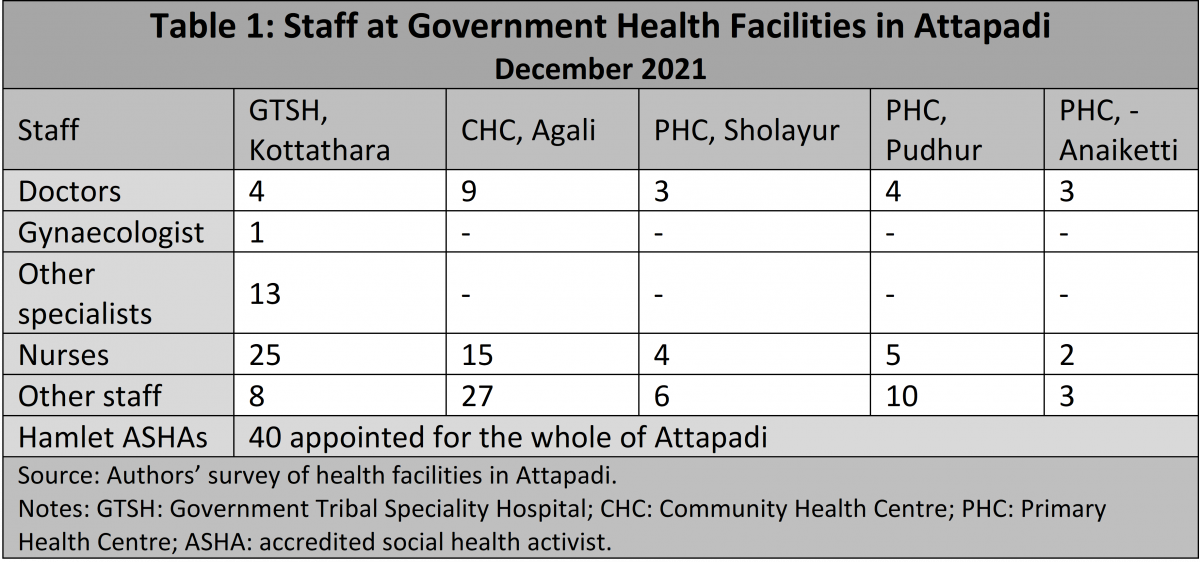
Attapadi has an extensive network of health facilities that are staffed by doctors, specialists, and other healthcare personnel (Table 1). All health personnel who opt to work in Attapadi are also given a special allowance amounting to 20% of their pay. In addition to these health facilities, there are two outpatient clinics operated by the Integrated Tribal Development Programme (ITDP) and a few private hospitals in Attapadi. Those requiring super-specialist care are referred to the EMS Cooperative Hospital in Perinthalmanna. All healthcare, whether inpatient or outpatient, is provided free of cost.
Despite such impressive levels of healthcare infrastructure, personnel, and resources, high levels of infant mortality have continued in Attapadi.
The Janani Janmaraksha Scheme of the state government, which began in 2013, gave Rs 1,000 a month to every pregnant woman for a period of 18 months starting from the first trimester if she completed all antenatal care (ANC) check-ups and delivered in a hospital. In 2018, the allowance was raised to Rs 2,000 a month. Despite such impressive levels of healthcare infrastructure, personnel, and resources, high levels of infant mortality have continued in Attapadi.
Alarm bells in 2021
Four successive infant deaths in November 2021 once again turned the spotlight back on Attapadi. Several key officials and the ministers in charge of health and tribal welfare from the government of Kerala visited Attapadi to study the situation and yet again announce measures to bring down infant deaths. One of the first announcements by the minister for tribal welfare was that a neo-natal intensive care unit (ICU) would be set up at the Government Tribal Speciality Hospital (GTSH) at Kottathara, Attapadi. Another step was a change in the referral hospital—from EMS Cooperative Hospital, Perinthalmanna to Government Medical College Hospital, Palakkad.
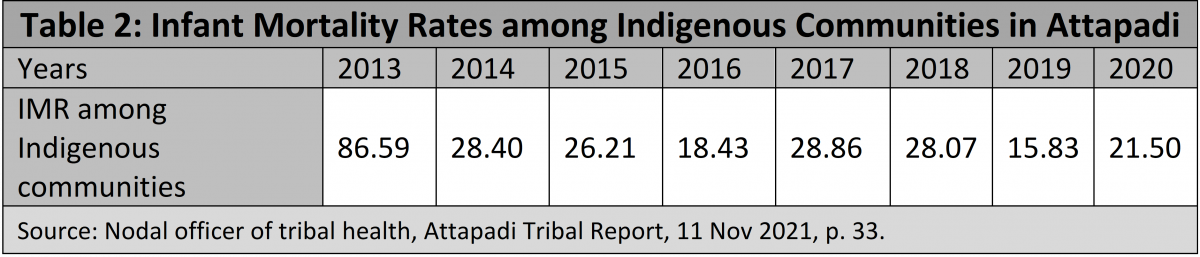
Some of the prominent politicians from the Opposition in the state who visited Attapadi in December 2021 also called for special packages to be implemented in the region. However, no thorough evaluation has taken place about why so many programmes launched since 2013 have not had the desired effect in Attapadi. A look at the infant mortality rate in Attapadi over the years (Table 2) shows that despite all government programmes, it has not improved all that much. These figures do not include still births among the indigenous communities.
Centralisation of services
Until now, healthcare in Attapadi was centred on the GTSH in Kottathara. Even antenatal care was delivered by one or two gynaecologists who were based in this hospital. For pregnant women living in remote villages, this meant several hours of trekking through the forest, climbing hills, and crossing the Bhavani or Varagar rivers before reaching a place where a jeep or a bus could take them to Kottathara. Depending on the season, the condition of the pregnant woman, and the availability of transport, this journey would take anywhere from eight hours to more than a day, just to go one way. As Kurumba Moopan, one of the village chiefs, said,
“In the past, a woman becoming pregnant was a cause of joy for the family. Now it is a reason for stress. That family must make these trips to Kottathara hospital monthly for ANCs. You have to go. If we don’t go, then someone will come asking why we are not following the schedule.”
The rationale for this approach was that a specialist screening all pregnant women would be able to detect any high-risk cases early and thereby prevent infant deaths. But as the results show, this approach has not worked as expected. There has been no attempt to decentralise healthcare by using the services of the various doctors and other healthcare personnel in the different health facilities in Attapadi.
Stigma, discrimination, and force
Most interventions so far have taken a paternalistic approach to the indigenous communities. Discussing problems with them and obtaining community consent for the various programmes have never been the state’s priorities. A classic example is how institutional delivery of babies at the Kottathara hospital has been implemented all these years. Instead of listening to the concerns of women who are afraid of leaving their homes and villages and using the antenatal period to build a rapport with them and win their trust, force and threats have been employed to achieve the desired results.
Instances of the police accompanying health workers to the villages to ensure that pregnant women are taken to the hospital to deliver their babies have done very little to build trust in the health system and its intentions. On numerous occasions, indigenous mothers have been accused of not knowing how to breastfeed their infants and thus harming them—stigmatising the poor women for no good reason.
That this has occurred in a state where the Channar revolt ... took place in the 19th century for the right of lower-caste women to cover their breasts worsens the irony.
A tell-tale sign was the installation of a statue depicting a woman breastfeeding her infant in the courtyard of the Kottathara hospital in 2019. Several young indigenous people in Attapadi pointed out that the woman in the statue was topless. While statues of mothers breastfeeding their children are commonly found on the premises of government hospitals across Kerala, unlike the one in Attapadi, those in other hospitals take great care to ensure that the mothers are depicted fully clothed. That this has occurred in a state where the Channar revolt, which was supported by social reformer Ayyankali, took place in the 19th century for the right of lower-caste women to cover their breasts worsens the irony. As Idi, an indigenous young person, put it,
“You have visited even remote villages. Have you seen any of our women topless? No, right? Then how did they make such a statue for this hospital? This shows the way outsiders perceive us; as savages who don’t wear clothes and roam around in forests.”
Top-down approach
Another example of the top-down approach that did not leverage the strengths of the indigenous communities was the Millet Village Scheme set up in 2017 to rejuvenate traditional agriculture in Attapadi. Every indigenous village in Attapadi has a traditional official known as the mannukaran (man of the soil), who is part of the indigenous village council. Traditionally, mannukarans had the responsibility of understanding the seasons, the nature of the soil in the location selected for cultivation that year, and choosing the right crop as well as the time it would be sown.

However, no discussions were held with the village chiefs (ooru moopans), mannukarans, or the village assemblies (oorukootams) before implementing this scheme. Village after village was drafted into this scheme in the belief that growing millets would solve the problem of malnutrition in Attapadi. In several cases, sowing under this scheme took place during the wrong season or in areas that were difficult to irrigate. However, the officials ticked off the targets that had to be met by the programme.
Alienation of land
Restoring traditional lands to the indigenous communities in Attapadi has been acknowledged at all levels as being critical to addressing their well-being. Every time there is a crisis there, everyone from experts to political parties discuss this issue in great detail. Alienation of land in Attapadi has occurred since the 1950s when outsiders, in connivance with local officials, produced documents that showed them to be the legal owners of the land. Today, most of the fertile land in Attapadi on the banks of the Bhavani and Siruvani rivers belongs to non-indigenous persons. Several special mechanisms set up to identify and return alienated traditional lands have so far not resulted in much being accomplished. But even a simple search on the internet for land in Attapadi will throw up the contact details of agents who offer several acres for sale. That this continues so openly when there are strict procedures and limits for any non-indigenous person who wants to buy a piece of land in Attapadi shows how the system is still broken and is loaded in favour of the powerful.
Land is not an asset to be owned by an individual but something that provides a connection to their ancestors, culture, and rituals.
For the indigenous people, their relationship with ancestral lands is an integral part of their identity. Land is not an asset to be owned by an individual but something that provides a connection to their ancestors, culture, and rituals. Any ownership is collective and meant for the entire community. For the indigenous communities in Attapadi, their ancestral land symbolises the umbilical cord that connects them to the earth and their identity (thoppulkodibendam).
The process of returning lands to the original indigenous owners in Kerala has an interesting and inequitable history. The Tribal Land Act enacted in 1986, which required all indigenous lands alienated after 1960 in the state to be restored to its original owners, was not implemented. In 1996, an amendment was brought to this Act that made only transactions of indigenous lands after 1968 illegal. Even under the amended Act, most applications for the restoration of land have been stuck for years in legal tangles, which have further impoverished indigenous claimants who have been spending time and money running from one authority to another to validate their claims.
One of the reasons stated by the state government for not implementing the 1986 Act and later amending it was the fear of large-scale violence between the settlers and the indigenous communities. That not returning alienated land to its traditional owners is nothing less than institutional, cultural, and structural violence against the most marginalised has been conveniently swept aside.

Another potential clue to the lack of political will to carry out land reforms lies in the current population of indigenous and non-indigenous people in Attapadi. According to the last census, the majority of those living in Attapadi today are non-indigenous. No political formation can take any drastic action such as returning all the lands that rightfully belong to the indigenous communities without losing the votes of the non-indigenous. In addition, the indigenous communitues in Attapadi are divided between the Left Democratic Front (LDF) and the United Democratic Front (UDF), and it does not make political or electoral sense to alienate the non-indigenous comunities.
Successful examples
Poor health among indigenous communities is a well-recognised phenomenon in different parts of India and several interventions have been carried out to successfully address this issue. Not far from Attapadi, the Tribal Health Initiative (THI) at Sittilingi in Dharmapuri district of Tamil Nadu empowers Malavasi women from the local community by training them as health workers to focus on primary health care.
But these sensible examples have neither been studied nor taken seriously in Attapadi, which continues to focus on centralised specialist care.
When we visited the THI in 2019, instead of its founders or doctors, it was a young indigenous community health worker who described to us how they addressed the high level of infant deaths and earned the trust of the community. She also pointed out how health was not to be limited to the hospital and that their farming initiative was begun to address both nutrition and livelihood issues, which are equally important. Like the THI, there are several initiatives across India where participatory community-based mechanisms have been successful in addressing the nutritional status of mothers and young children. But these sensible examples have neither been studied nor taken seriously in Attapadi, which continues to focus on centralised specialist care.
Way forward
Kerala has several firsts in social justice and development to its credit. The inability of the state and its institutions to achieve the same in Attapadi shows that islands of inequity continue to exist in “God’s own country”, as Kerala brands itself. One of the first steps that the state government should take is to engage with the indigenous communities and their institutions as first among equals. Whether it is addressing malnourishment or improving antenatal care, experts and officials need to recognise that listening to the indigenous communities, integrating their worldview and knowledge, and working with them as allies are important first steps if these programmes are to have the necessary impact. Development that is inclusive should build on the strengths of the indigenous communities and come up with solutions that are meaningful to their culture and traditions.
A failure to do so leads to several initiatives that underperform and, in the process, not only waste precious resources, but also, more importantly, require the stripping away of the indigenous identity to benefit from these initiatives. We are aware that substantial change will not happen overnight. But it requires a start by setting up mechanisms and processes within the various departments that function in Attapadi to ensure that their activities are culturally safe and engage meaningfully with the indigenous communities. Implementing the Panchayats (Extension to Scheduled Areas) (PESA) Act, 1996 is another step that needs to be taken to have a governance mechanism that integrates the traditional systems of indigenous communities.
Restoring alienated land is more a political issue than a legal one. It requires all political parties in Kerala to step up to the challenge and find a solution rooted in social justice. Merely setting up more committees will only ensure that the indigenous claimants are once again stuck in legal quagmires that will take years to resolve. Unless a fundamental shift occurs, setting up hospitals, posting more doctors, or growing millet will not reduce the underlying inequalities that give rise to conditions that foster poor health and lead to the death of infants in Attapadi.





Are there no medical reasons?