India has the largest adolescent population, that is, those between the ages of 10 and 19, in the world. In 2023, 250.8 million people in India—nearly one-fifth of the country’s population—are adolescents. India’s achievement of many of the United Nations’ Sustainable Development Goals and their targets will depend a lot on the development and well-being of these adolescents, directly or indirectly.
Since the 1994 International Conference on Population and Development (ICPD), and especially since the turn of this century, policy and programme commitments to address adolescents’ sexual and reproductive health and rights (ASRHR) have expanded in India. How far have we come in promoting sexual and reproductive health and rights of adolescents?
Drawing on data largely from various rounds of the National Family Health Survey, this article explores India’s progress in promoting ASRHR over the course of this century and discusses additional actions that need to be taken to enable all adolescents to make a safe and healthy passage to adulthood. Specifically, this article focuses on progress in reducing selected vulnerabilities faced by adolescents, particularly adolescent girls—child marriage, unsafe sex, early and unintended pregnancy, and violence and sexual coercion. It is acknowledged that sexual and reproductive health and rights encompass many more components than what this article focuses on.
Child Marriage
Forty-five years have elapsed since the enactment of the Child Marriage Restraint Act that prohibited marriage to a girl before she reaches the age of 18 and to a boy before he reaches the age of 21. Age at marriage for women has undergone a secular increase and the prevalence of child marriage has declined by half over the course of this century in India.
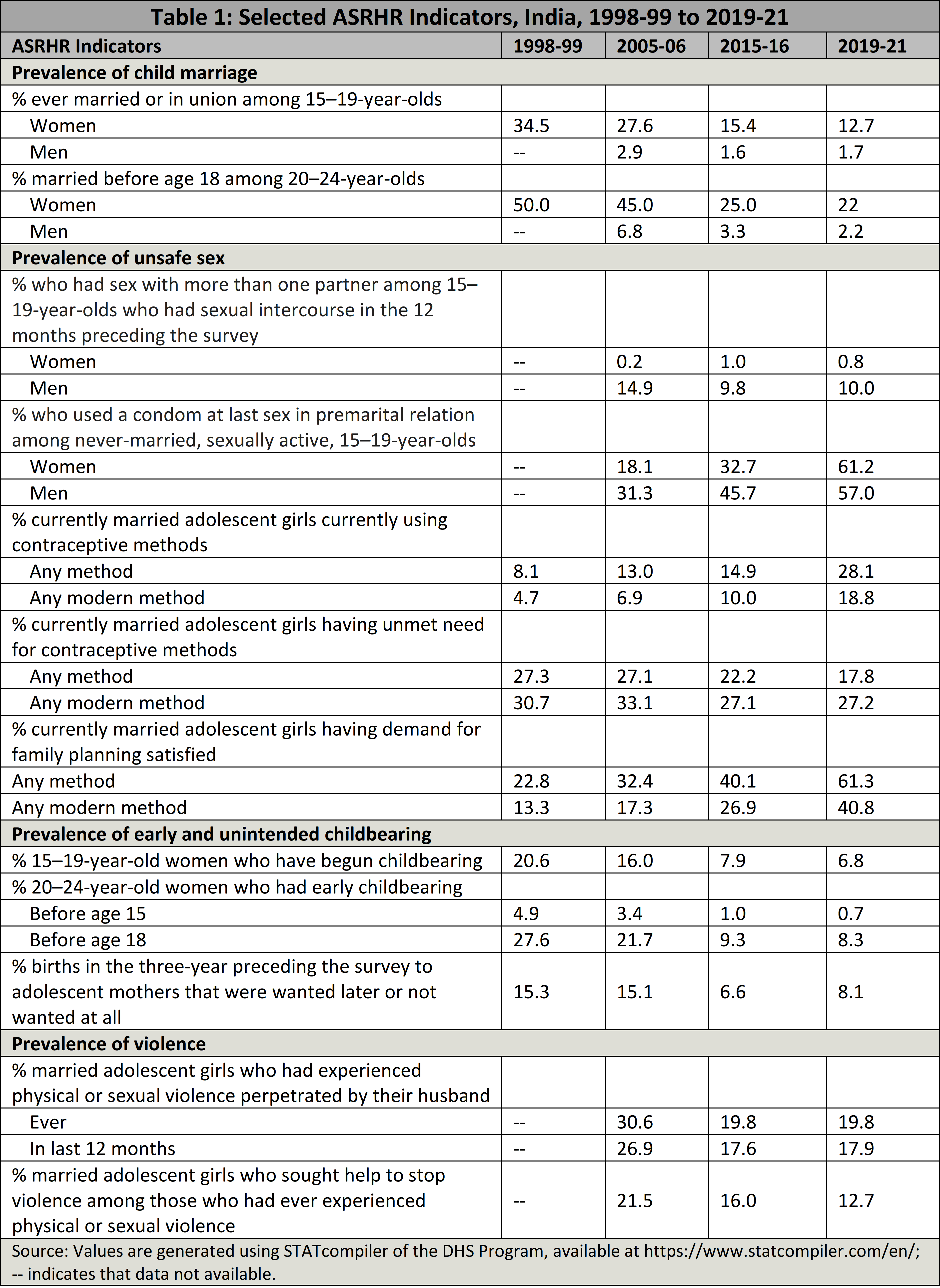
Yet, one in eight adolescent girls aged between 15 and 19 were ever married as recently as in 2019-21 (Table 1). And almost a quarter of all women aged 20-24 were married by age 18, which means that roughly 14 million young women were married as children.
Progress in reducing child marriage among women has been uneven. Poor, rural and poorly educated young women continue to experience early marriage. For example, as many as 46% of young women aged 20-24 with no education were married before they were 18 in 2019-21, compared to 3% of those with more than secondary education. Between one in three and two in five young women were married by 18 years in states such as Assam, Jharkhand, Bihar, Tripura, and West Bengal.
India will also not meet the SDG for the elimination of forced marriage, that is, marriage entered without “full, free, and informed consent” by 2030.
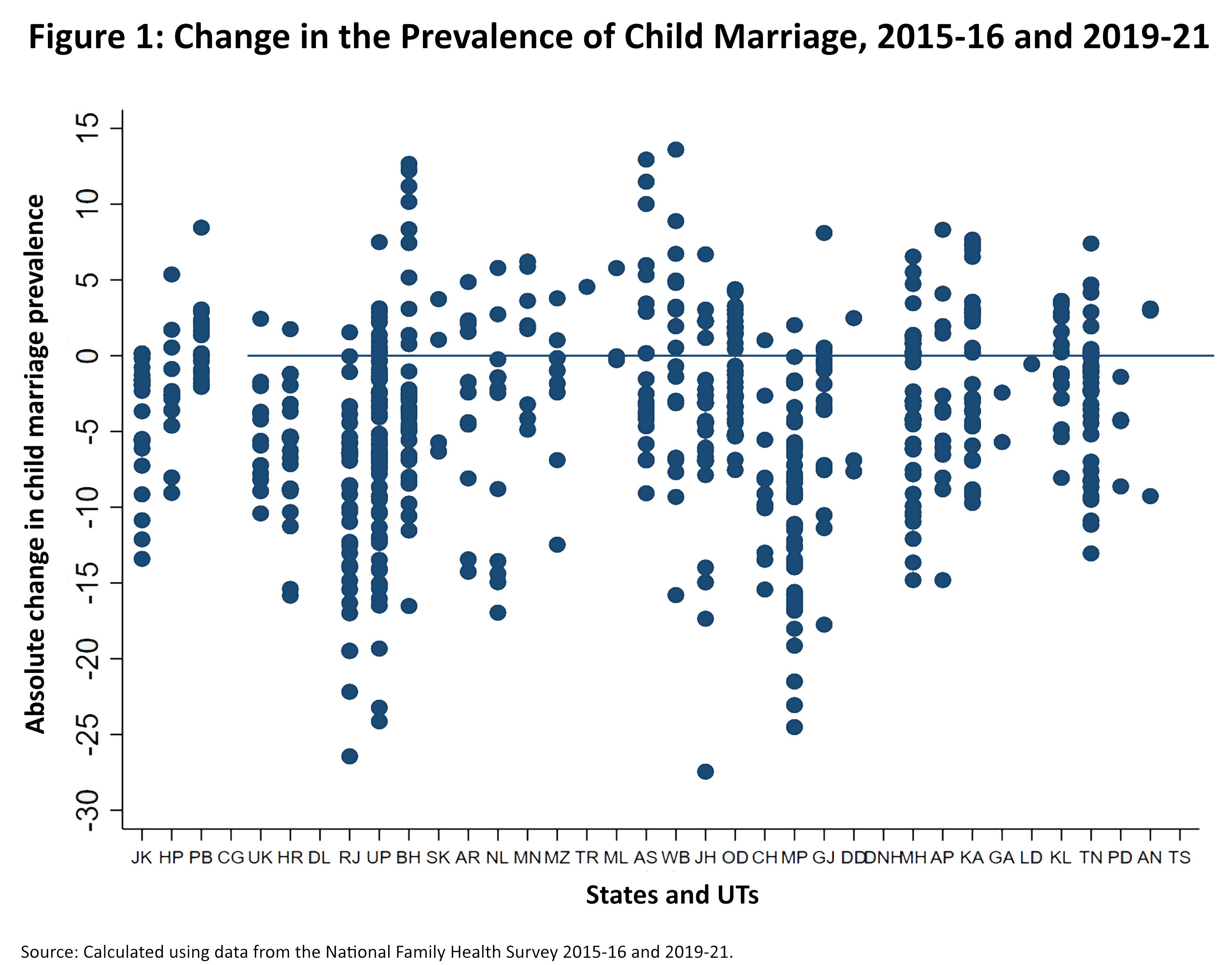
A comparison of change in the prevalence of child marriage between 2015-16 and 2019-21 shows that while it declined in several districts, it increased in several others during the inter-survey period (Figure 1). A modelling exercise reports that just 26 of 707 districts had achieved the SDG target of eliminating very early child marriage (below the age of 15), while 375 districts were on track and the remaining 306 districts were off track.
As far as marriage below the age of 18 was concerned, 168 districts were on track, while the remaining 539 districts were off track. This modelling exercise notes that India is likely to achieve the SDG target of eliminating child marriage before the age of 18 only in 2045 (Subramanian et al. 2023: 9). India will also not meet the SDG for the elimination of forced marriage, that is, marriage entered without “full, free, and informed consent” by 2030.
Evidence from state-level studies show that although there has been an increase in the proportion of married girls reporting that they had a chance, before marriage, to meet or talk with their fiancé in private and a decline in the proportion reporting that they met their husband for the very first time on the wedding day, family-arranged marriages continue to be the norm, with or without the girl’s involvement (Jejeebhoy 2019: 10).
Unsafe Sexual Relations
Notable proportions of sexually adolescent boys report multiple partnerships, though sexually active adolescent girls rarely report this. Nationally, among adolescents who had engaged in sex in the past 12 months, one in 10 boys had engaged in sex with more than one partner, while 1% of girls reported so (Table 1).
Condom use within pre-marital relationships has increased over time. But just 62% of adolescent girls and 57% of adolescent boys aged 15-19 who had engaged in pre-marital sex in the past 12 months had used a condom for the last sexual intercourse in 2019-21. Condom use in pre-marital relationships was lower among poor, rural, poorly educated, and socially disadvantaged adolescent girls and boys than others.
Among married girls too, contraceptive use remains limited. The use of modern methods of contraception among married girls has increased by three times over the course of this century. Even so, fewer than one in five married girls aged 15-19 used any modern contraceptive method in 2019-21. Differentials were notable—adolescent girls were only two-thirds as likely as young women (20-24) to use contraceptives.
[I]ndia may take till 2046 to meet the SDG target of demand satisfied for 99% of women of reproductive ages.
Moreover, more than a quarter of girls reported an unmet need for modern methods of contraception, signifying a large gap between married girls’ reproductive intentions and their contraceptive behaviour. Further, the pace of decline in unmet need among married girls was small—just 0.2 percentage point per annum over the course of this century (30.7% in 1998-99 to 27.2% in 2019-21). Although the proportion of demand for family planning that is satisfied by modern methods, or “demand satisfied”, among married girls has increased by more than two times over the course of this century, just 41% of married girls had their demand for family planning satisfied by a modern method in 2019-21.
This highlights that the current efforts by the government and the broader family planning community in meeting the commitment to make family planning services accessible to all adolescent girls who want them are far from adequate. The modelling exercise reports that India may take till 2046 to meet the SDG target of demand satisfied for 99% of women of reproductive ages.
Early Childbearing
Early childbearing has declined by two-thirds over the course of this century in India. Even so, 7% of girls aged 15-19 were already mothers or were pregnant with their first child, which means there were about 4 million teenage mothers in 2019-21. And 8% of young women aged 20-24 had their first baby before they were 18 years of age.
Between one-tenth and one-quarter of young women had their first birth by age 18 in states such as Andhra Pradesh, Arunachal Pradesh, Assam, Bihar, Jharkhand, Meghalaya, Tripura, and West Bengal. Rural young women were almost twice as likely as the urban to have their first birth by age 18. Less educated young women, those belonging to poorest households, and those belonging to Scheduled Tribes were more likely than others to have given birth before they were 18 years of age. For example, 20% of young women with no education compared to less than 1% of those with more than secondary education had their first birth before age 18. The modelling exercise reports that India is likely to meet the SDG of eliminating teenage pregnancy by 2039. Early childbearing is accompanied by too close childbearing for many—65% of births to adolescent girls aged 15-19 occurred less than 24 months since the preceding birth in 2019-21.
Because of early initiation of childbearing, inadequate care during pregnancy and childbirth, and limited access to safe abortion, maternal causes claim the lives of many adolescents in India.
High rates of unintended pregnancy and abortion are also observed among adolescents. It is estimated that of the two million pregnancies that occur among adolescents in India each year, 53% end in abortion, resulting in 930,000 abortions annually. An estimated 78% of abortions among adolescents are unsafe (Murro et al. 2021: 4).
As many as 8% of births to adolescent mothers in the three years preceding the survey were wanted at a later time or not wanted at all in 2019-21. Over the course of this century, births that were wanted at a later time or not wanted at all were almost halved in India (15% in 1998-99 to 8.1% in 2019-21).
Because of early initiation of childbearing, inadequate care during pregnancy and childbirth, and limited access to safe abortion, maternal causes claim the lives of many adolescents in India. Adolescents aged 15–19 accounted for 6% of maternal deaths in 2018-20 (Office of the Registrar General 2022: 4).
Although neonatal and infant deaths among children born to adolescent mothers have declined over the course of this century, almost one in 40 new-borns to adolescent mothers died during the neonatal period (neonatal mortality rate of 24.3 deaths per 1,000 live births) and one in 28 infants to adolescent mothers died before their first birthday (infant mortality rate of 36.2 per 1,000 live births).
Sexual Coercion and Violence
Violence against girls takes many forms. Violence against girls is perpetrated largely by husbands and partners, starts early in relationships, and is a reflection of the inegalitarian gender norms that are pervasive in most settings. One in five ever-married adolescent girls had experienced physical or sexual violence perpetrated by their husband in 2019-21, down from one in three in 1998-99.
Sexually experienced unmarried adolescent girls also report non-consensual, including forced, sexual encounters. For example, in a state-representative study of adolescents in Bihar and Uttar Pradesh, 8-11% of unmarried girls aged 15-19 reported ever experiencing non-consensual sexual touch, including attempts to force sex on them, and 4% of unmarried girls reported a forced sexual encounter ever in life (Santhya et al. 2017a: 218; 2017b: 216). The modelling exercise reports that India may take till 2090 to meet the SDG target of eliminating physical or sexual violence perpetrated by intimate partners.
Adolescent girls and boys are generally uninformed or misinformed about their bodies, sexuality, and health promoting behaviours.
In short, the sexual and reproductive health and rights situation of adolescents in India has undoubtedly improved. Nonetheless, progress has been slow and uneven, and wide regional and sub-population differences exist. Adolescents residing in rural areas, with limited education, and belonging to economically disadvantaged households or socially excluded ethnic groups are particularly vulnerable.
Several factors, most importantly, lack of knowledge, agency, services tailored to adolescents’ specific needs and situations and a supportive environment, have compromised ASRHR. Adolescent girls and boys are generally uninformed or misinformed about their bodies, sexuality, and health promoting behaviours. For example, just 18% of girls and 26% of boys aged 15–19 displayed comprehensive knowledge about HIV in 2019-21.
While awareness of at least one modern contraceptive method is universal among married girls and boys (99%), in-depth knowledge remains limited. Adolescent girls, especially those who are most disadvantaged, are socially isolated and denied agency, placing them at risk for poor sexual and reproductive health and rights SRHR outcomes. For example, just 51% of married girls participated in making decisions related to their own healthcare, major household purchases, and visiting their family or relatives in 2019-21.
Access to SRH services is limited for both married and unmarried adolescents. Three in five adolescent girls reported problems such as getting permission to go for treatment, getting money for treatment, distance to health facility, finding someone to go with them and concerns about lack of female providers in seeking healthcare in 2019-21. Although adolescents require safe and supportive families, safe and supportive schools, and positive and supportive peers, the environment falls short of meeting adolescents’ needs and protecting their rights.
There is also strong global evidence of the positive effects of a comprehensive sexuality education delivered to school-going adolescents.
Available evidence from India and elsewhere suggests a host of promising practices to protect ASRHR and enable adolescents’ empowerment (Jejeebhoy 2017: 38-45). Gender transformative life skills education programmes implemented in a variety of settings in India have shown positive effects in raising adolescents’ awareness of ASRHR matters, changing their gender role attitudes, and building their agency. A few have shown positive effects in delaying marriage and childbearing, promoting birth spacing, or reducing violence against girls.
There is also strong global evidence of the positive effects of a comprehensive sexuality education delivered to school-going adolescents. Similarly, programmes that provide safe social spaces for vulnerable adolescent girls and some combination of “assets” such as knowledge about health and sexuality, social and economic rights, financial literacy and savings, and self-protection planning and resources such as health services available in the community have shown promising results.
Making health services adolescent friendly, along with training service providers about the needs of adolescents and how to provide services to them in supportive, non-threatening ways, is observed to increase service use. Parenting programmes, although commonly implemented in high-income countries, have found promising results. It is critical that investments in adapting and scaling up these strategies are stepped up to help all adolescents make a safe and healthy passage to adulthood.
K.G. Santhya is an economist and demographer who has conducted studies on rights of youth, gender equity, women’s empowerment, reproductive health, and gender-based violence. She currently works as an independent researcher; prior to this, she held positions as Senior Associate and Associate at the Population Council’s office in New Delhi.